
Fever Management In Toddlers With Chronic Illness
Introduction
If you’re trying to manage a toddler’s fever when they also have a chronic condition, the main rule is boring on purpose: confirm a real temp with a reliable method, treat discomfort (not just a number), and escalate fast when the overall picture looks wrong or your child’s condition has a “don’t wait” pathway.
In most clinics, a true fever is 100.4°F (38°C) or higher on an accurate reading. That’s it. The rest is context. A temp is a data point, not a verdict, and with medically complex kids it’s a data point that sometimes carries more risk than it does in an otherwise healthy toddler. The scale of this isn’t small, either. Pediatric chronic conditions have climbed to nearly 30% over the last two decades, which means lots of families are living this loop, not just the “rare cases” you get brushed off with at urgent care, as the figures in a UCLA Health summary of pediatric chronic disease prevalence make pretty plain.
Also, quick throat-clearing (because it matters): I’m talking about toddlers roughly 1 to 3 years old. If you’re dealing with a younger infant, different rules kick in, and the tolerance for waiting drops hard.
What counts as a fever by age and method
Temperature cutoffs
For toddlers, the headline cutoff is still 100.4°F. The messiness comes from where you measure. Rectal is closest to core body temp; oral is solid but toddlers rarely cooperate; ear and forehead can be good with good technique; armpit is a fuzzy estimate.
Here’s the clean way I think about it:
Method (toddlers) |
When I trust it |
What I do with borderline numbers |
Rectal |
Best accuracy if you truly need precision |
Treat ≥100.4°F as real |
Oral |
Only if your kid can keep lips sealed and not chew the probe |
Recheck if it seems “off” |
Ear (tympanic) |
Works well with correct placement and the right size tip |
Repeat in the other ear |
Forehead (temporal) |
Great for screening, less great for courtroom drama |
Confirm with ear/rectal if the reading drives decisions |
Armpit |
Low-stakes, not a deciding tool |
Assume it may under-read |
One note for chronic conditions: some specialty teams set lower “call us” thresholds than general pediatrics. Sickle cell disease is the classic example. Many hematology programs treat 100.4°F as an urgent trigger because delays can be deadly with encapsulated bacteria like S. pneumoniae. You’ll see that spelled out in a SSM Health sickle cell fever guideline.
When “high” matters
A toddler can look fairly okay at 103°F, and another can look scary at 101°F. Still, higher numbers do matter in a few practical ways.
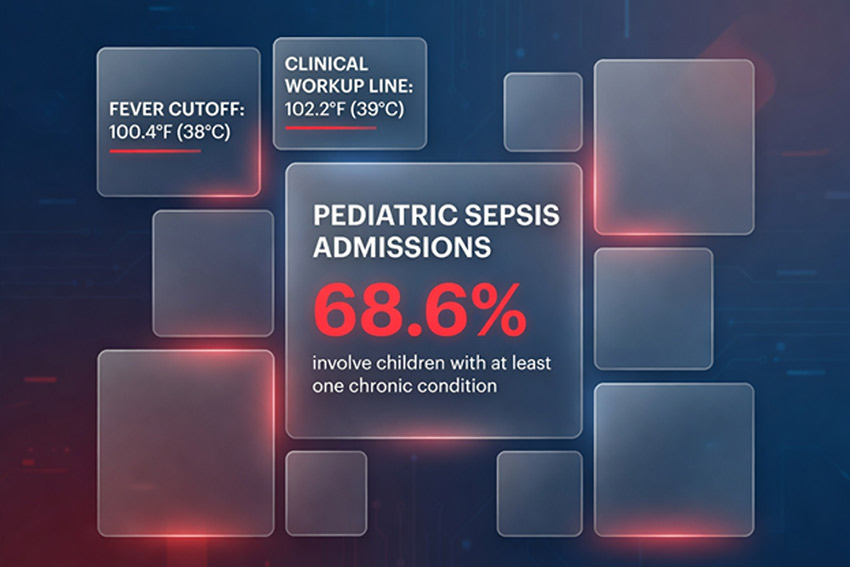
First, ≥102.2°F (39°C) often shows up in clinical algorithms as a line where clinicians think harder about workups when there’s no obvious source, as in this Texas Children’s guideline for fever without localizing signs.
Second, when you have a kid with a central line, immunosuppression, a history of sepsis, significant heart or lung disease, or sickle cell disease, the concern isn’t “high temp equals brain damage.” It’s that the same spike could represent bacteremia, pneumonia, meningitis, an influenza complication, or an early sepsis curve that doesn’t care about your calendar.
That’s not drama. It’s statistics. A large analysis on NIH’s PMC reports 68.6% of pediatric sepsis hospital admissions involve kids with at least one chronic condition. That’s the risk profile shift in one ugly number.
Why the number shifts
Temps bounce because the hypothalamus is acting like a thermostat that just got a new setting. Cytokines rise, the set-point rises, shivering kicks in, blood vessels constrict, and suddenly your toddler feels like a space heater even before the reading catches up.
It also shifts because toddlers are chaos engines. They run, they cry, they nap under a fleece blanket they refuse to surrender, they drink two ounces and declare themselves done with all liquids forever. So you can see a real spike and a fake spike in the same night.
Take a temperature you can trust

Best tools by age
If you want one purchase that doesn’t betray you, it’s a decent digital thermometer you can use correctly in the ear or rectally, plus a forehead scanner for quick checks.
For toddlers with chronic disease, accuracy isn’t about being obsessive. It’s about not wandering into the emergency department with a story that starts with “I think it was kind of high?” and ends with a full workup because no one can anchor the timeline.
Step-by-step technique
For ear readings, the technique is half the game. You want the canal aligned, the probe seated, and a calm repeat if the number surprises you.
Rectal (if you’re doing it) should be gentle, lubricated, and shallow. If that makes you nervous, good. Nervous people follow instructions.
Forehead scanners like a clean, dry forehead and a slow pass. Sweat and recent baths distort things. So does taking it right after they’ve been lying on one side with a warm cheek smashed into a pillow.
Recheck timing
My personal anti-spiral move is to stop treating the thermometer like a stock ticker. I take a reading, do comfort care, then recheck on a schedule. Not five minutes later. Not “just to see.” Kids don’t improve on demand.
If you gave acetaminophen or ibuprofen, expect the effect window to show up over 30 to 60 minutes, not instantly.
What fever means inside the body
What fever means inside the body
Immune purpose
A higher body temp can slow down some pathogens and boost parts of the immune response. So the goal isn’t “zero fever forever.” The goal is: keep your kid safe, hydrated, and monitored while the immune system does its job.
This is why a toddler can be warm and still be okay. Alert enough. Breathing normally. Drinking. Peeing.
Common causes
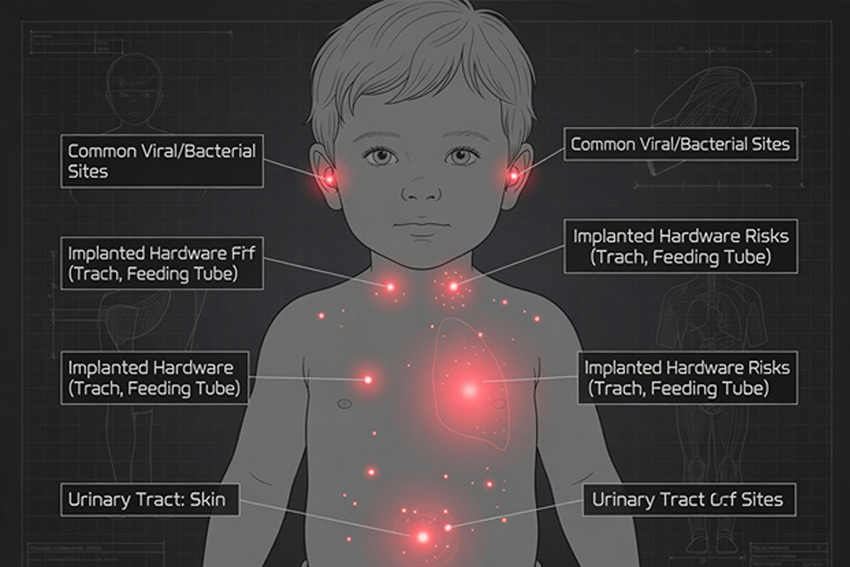
Viruses dominate. RSV (syncytial virus), covid 19, influenza, adenovirus, all the daycare greatest hits. Some bacterial infections still matter a lot, especially ear infections, pneumonia, urinary tract infections, and skin infections.
If your toddler has a trach, a feeding tube, a urinary catheter, eczema that cracks and bleeds, or any implanted hardware, the list of possible entry points for germs gets longer. This is where “same symptoms, different stakes” becomes real.
When fever misleads
Autoinflammatory conditions and periodic fever syndromes are the classic mind-bender. PFAPA gets the most casual mentions online, but the umbrella is bigger, and a careful review on NIH’s PMC describing periodic fever incidencepegs these syndromes at about 2.3 per 10,000 kids under five each year. Not common, not mythical either.
Post-op spikes can be their own weird category too. One AAP Hospital Pediatrics analysis of postoperative fever complexity reported rates up to 35.2% after major surgeries in kids with chronic conditions, which is a fancy way of saying the body throws tantrums while healing.
So yes, warmth can mean infection. It can also mean inflammation, meds, vaccines, heat, dehydration, or a post-surgical response. That’s why you track the whole picture.
Use a calm 30-minute home routine

I’m with you on the emotional reality. Toddler fever is ruin-your-night energy. I used to hover and recheck constantly and pretend the next reading would deliver emotional closure. It never did. What helped was switching to a tight, boring routine that I could follow even while my anxiety was yelling.
Comfort first checklist
This is the “next 30 minutes” protocol I run, and I’m not trying to be chill, I’m trying to be effective:
1. Take a reliable temp and write down the time and method.
2. Look at behavior: responsiveness, breathing, color, hydration, pain.
3. Light clothing, cool room, no bundling.
4. Offer fluids in small, repeatable amounts.
5. Meds only if they look miserable or can’t rest.
6. Recheck on schedule, not compulsively.
For cooling, I’ll do lukewarm wiping if it helps comfort, and I will not do cold baths, ice packs all over, or any “home hacks.” Medical groups keep warning people not to do alcohol baths for a reason, and I like my risk decisions to be adult ones, not TikTok ones, which is part of why I keep a single mental bookmark to this Children’s Health guidance on what to do when your child has a fever.
Hydration targets
Hydration is the sneaky decider. A toddler can run hot and still be okay if they’re drinking and peeing. When they stop drinking, the whole situation gets harder: higher heart rate, more irritability, higher risk if you use ibuprofen, less margin for error.
You don’t need a perfect ounces-per-hour spreadsheet. You need evidence of intake and output. Wet diapers or bathroom trips. Tears. Moist mouth. Some willingness to sip.
If you’ve got a kid with kidney disease, complex cardiac disease, or fluid restrictions, follow your specialty plan. This is where “drink more” is not universally safe.
Monitoring log
A simple log beats memory every time. Time, reading, method, meds (dose and time), fluids, pee, key symptoms (breathing, rash, pain, sleepiness). If you end up calling the pediatrician or going in, you look calm and credible, and clinicians can spot trends faster.
Use acetaminophen or ibuprofen safely
Treat discomfort, not the number, unless your care team told you otherwise. Some kids with neurologic issues, prior febrile seizures, or specific cardiac conditions do better when you’re proactive, but that’s a clinician-guided call.
In general dosing terms for toddlers:
Acetaminophen is usually dosed by weight every 4 to 6 hours, with a daily max. Ibuprofen is usually every 6 to 8 hours and tends to be avoided in dehydration, kidney disease, or certain GI issues. Never use aspirin in kids because of Reye syndrome risk.
My personal rule is: I don’t “stack” meds like it’s a hobby. I write down the dose, I set a timer, I don’t freestyle. If you’re the kind of person who second-guesses yourself mid-crisis, you need that written plan more than you need another parenting podcast.
If you want a reality check on why routines matter, read one raw parent thread where someone describes being traumatized after febrile seizures and then spiraling every time their toddler runs hot, because it’s painfully familiar and oddly grounding in a bleak way, like this discussion about anxiety over toddler fever after febrile seizures.
Know when to call or go now
This is where chronic conditions change the whole equation. If your kid has sickle cell disease, for example, lots of pathways say: any temp at or above 100.4°F is urgent, and antibiotics should be started quickly. CHOP’s clinical pathway for sickle cell disease with fever even bakes in a goal of broad-spectrum IV antibiotics within 60 minutes of arrival. That’s not because hematologists are paranoid. It’s because the pathogens can move fast, and the consequences are brutal.
The same urgency logic can apply to immunosuppression (steroids, chemo, biologics), transplant, central lines, complex congenital heart disease, significant chronic lung disease, metabolic disorders, and kids with prior sepsis.
Use this table like a gut-check, not a substitute for your own plan:
Situation |
What I’d do |
Trouble breathing, blue/gray color, severe lethargy, hard to wake, stiff neck, new confusion |
Emergency care now |
Dehydration signs (no pee for 8+ hours, very dry mouth, no tears, persistent vomiting), uncontrolled pain |
Call urgently, same-day evaluation |
Petechiae/purple rash, severe headache, persistent inconsolable crying |
Emergency care now |
First seizure, seizure lasting >5 minutes, repeated seizures in 24 hours, or breathing problems during it |
Emergency care now |
Sickle cell disease with temp ≥100.4°F (even if “acting fine”) |
Follow hematology pathway, urgent evaluation |
Immunocompromised or central line with new fever |
Call your specialist or go in as directed |
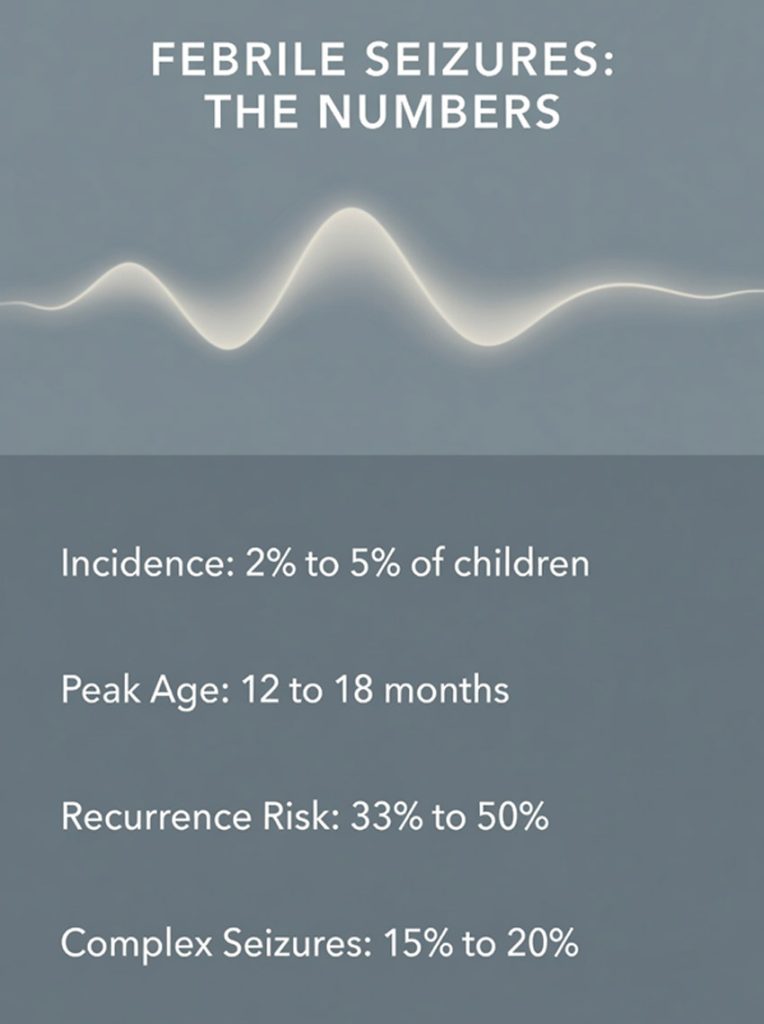
If seizures are part of your story, a few numbers help you think straight. Febrile seizures happen in 2% to 5% of kids in the US and Europe, peaking around 12 to 18 months, per StatPearls’ clinical overview. Recurrence after an initial event can be 33% to 50%, according to a Johns Hopkins clinical pathway. Complex febrile seizures (longer than 15 minutes or recurring within 24 hours) make up about 15% to 20%, per a review hosted on NIH’s PMC. Most kids outgrow them, and the Child Neurology Foundation’s overview notes roughly 1 in 25 children will have at least one.
What to do in the moment is simple and not negotiable: lay them on their side, keep the airway clear, don’t put anything in the mouth, time it, call emergency services if it hits five minutes or if breathing looks off.
One more escalation line that gets ignored: prolonged fever. A multicenter study in Archives of Disease in Childhood found 10.6% of febrile children had a prolonged fever of five days or more, which correlates with higher serious bacterial infection risk. If you’re hitting day five, you’re not “being extra” by calling.
And if you’re parenting a medically complex toddler and you feel dismissed, keep this in your back pocket: while only about 5% of chronic pediatric cases are classified as severe, that group accounts for 33% of total hospital days, per an analysis on NIH’s PMC. Systems get optimized around averages. Your kid might not be the average.
If you want a single, mainstream, non-dramatic page that also warns against unsafe home treatments like rubbing alcohol, I like that Nationwide Children’s Hospital overview of fever keeps it blunt.
FAQ
Should I wake my toddler to give medicine? If they’re sleeping comfortably and breathing normally, I usually let sleep do its job. If their condition has a specialist instruction to treat aggressively, follow that plan.
What if the temp isn’t coming down with meds? A partial response is common. The goal is comfort and hydration, not hitting 98.6°F on command. If they’re getting more lethargic, breathing is changing, or they’re not drinking, that’s when the plan shifts to calling or going in.
Does a higher temperature mean a bacterial infection? Not reliably. Viruses can spike high. Bacterial infections can present with modest temps. Clinicians use the whole picture, sometimes labs like CBC, blood cultures, urinalysis, CRP, and imaging depending on symptoms and risk.
How does covid 19 change this? It doesn’t change your home routine much. It changes exposure assumptions, and it may change how fast you test and isolate, especially if someone high-risk lives with you. Escalation is still about breathing, hydration, mental status, and your toddler’s underlying disease.
Conclusion
The trick, if there is one, is refusing the two classic traps: treating the number like a courtroom sentence, or pretending you’re “chill” when your kid is medically complex. A storm-warning mindset works better. Confirm the temp with a method you trust, run the same calm 30-minute routine every time, use acetaminophen or ibuprofen with written-down dosing when comfort demands it, and know your red lines for calling a clinician or heading in. That’s not overreacting. That’s competent parenting under pressure.
